
These lesions are most often associated with papules or even pustules – erythematous lesions containing purulent fluid – that appear later in the course of rosacea.
It is a chronic skin condition that appears on various parts of the face such as the nose, cheeks, chin and forehead – the area around the mouth remains unaffected.
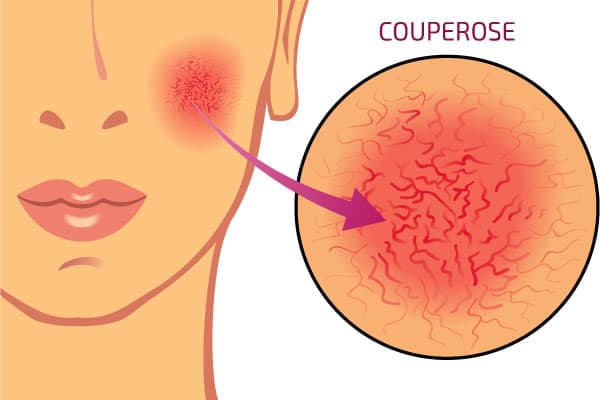
Spider veins are characteristic of rosacea ©rob3000/123RF
Although it is very rare, it can also occur on the eyelids and eyes.
Its subjects are usually middle-aged people with fair skin who blush easily. It often appears around the age of 30, but it can appear earlier, starting at age 20.
It is more severe in men, but more common in women. Men are more likely to develop rhinophyma, a very advanced stage of rosacea characterized by a red, bumpy, swollen nose.
When left untreated, rosacea worsens over time. Its symptoms usually progress in a cyclical fashion, with alternating periods of worsening and periods of remission.
Causes of rosacea
To date, the exact causes of rosacea have not been determined.
The various existing theories are based on the fact that this dermatosis combines a vascular component with inflammation. It is said to be a disruption of the immune system in the skin; this creates an abnormal reaction of the skin to the sun.

The origins of rosacea are a bit of an enigma
Also, the warmth and redness are due to an excessive dilation of the blood vessels in the face, reflecting a hyperactivity of these vessels.
Hypotheses also attribute rosacea to parasitic activity involving mites of the Demodex folliculorum type on the skin and other bacteria such as Helicobacter pylori affecting the stomach. However, these assumptions about microorganisms have never been proven.
Other popular beliefs point to rosacea being caused by alcohol. Although this is not true, alcohol intake (even moderate) can worsen rosacea.
In fact, any factor that can create flushing can make acne rosacea worse. Like alcohol, other factors include: stress, exercise, hot drinks, consumption of spices, high or low temperatures…
It should also be noted that the continuous application of corticosteroid-based creams on the face can lead to skin lesions similar to those of rosacea. In such cases, if the cream has been prescribed for treatment, it should be stopped.
Stages of rosacea progression
The progression of rosacea isnot the same in all individuals. There are four subtypes of rosacea.
Although these subtypes are considered stages in the progression of the dermatosis, many people never see rosacea progress to the final stage.
Instead, most people with rosacea have a combination of the subtypes. Thus, it is very complicated to predict a specific course of the disease.
The subtypes of rosacea are as follows:
Erythematotelangiectatic rosacea
This vascular form is usually the primary symptom of rosacea. It manifests as flushing or flushes that disappear after a few minutes (such flushes can occur on skin already affected by spider veins).
These flushes appear after sudden changes in temperature, consumption of hot drinks or spicy foods, sun exposure, etc.
Papulopustular rosacea
Here, in addition to rosacea, small, red, solid pimples (papules) or purulent pimples (pustules) appear in flare-ups and over several weeks.
Most often, this subtype is accompanied by hot flashes, but it is also possible that facial edema occurs. The latter is, however, very rare.
Phymatous rosacea
95% of cases of this subtype are observed in men. This hypertrophic form affects the nose more.
Here, the pores dilate, the skin of the nose thickens forming nodules. As a result, the nose is deformed. This is called rhinophyma.
Ocular Rosacea
More than half of those with rosacea experience this subtype. Here, blepharitis (inflammation of the eyelids), conjunctivitis (redness of the conjunctiva), dry eyes (xerophthalmia) and even keratitis (corneal disease) occur.
In this case, the eyes become irritated and feel like there is a foreign body in the eye.
Here’s a infographic summary of the different subtypes of rosacea :
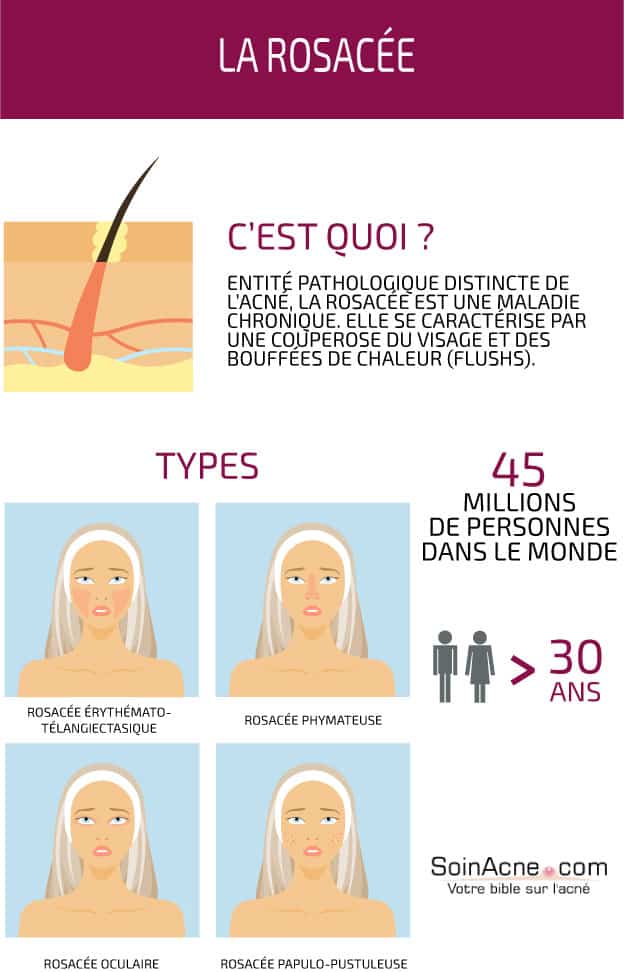
Rosacea subtypes, characteristics and statistics ©moremar/123RF
People at risk for rosacea
As noted at the beginning of this article, women are much more affected by this dermatosis than men. The number of women with rosacea is almost double the number of men.
Rosacea sufferers are often fair or pale skinned individuals. The disease is common among Irish, Scottish and Scandinavian descendants. By way of consequence, in France, it is highly described in Bretons.
In addition, let’s point out that there are families where people with rosacea are noted across generations. Although the genetic link has never been proven, it is considered that hereditary factors could increase the risk of being affected by rosacea.

Women have more rosacea than men ©artemidapsy/123RF
Rosacea treatment
Topical and general treatments exist for the different types of rosacea.
Antibiotics and antifungals are used to remove pus and red spots.
For nasal deformities, it is common to treat with remodeling lasers (CO2, erbium) and, for redness, with vascular lasers.
It is necessary to follow the attack treatment with a maintenance treatment and avoid factors that aggravate the dermatosis.
More information on laser treatments is available from our page on acne treatments.
Pimples treatment
As we just announced, there are both topical and systemic treatments.
Topical treatments
For moderate rosacea, metronidazole at 0.75% can be effective. It can be found as a gel, cream or emulsion (Rozex®, Rozacrème®…).

Creams and gels are among the topical treatment solutions for rosacea ©studiostoks/123RF
For more severe rosacea, it is possible to combine metronidazole with oral antibiotics. Treatment can be continuous or intermittent.
Topical erythromycin, benzoyl peroxide, topical clindamycin (Dalacin T Topic®), and azelaic acid 15% gel (Finacea®) are also very effective against red pimples.
However, it should be noted that only azelaic acid is recommended (in addition to metronidazole) by the French College of Dermatology.
Local creams with corticosteroids should be avoided: although they reduce rosacea and inflammation rapidly, they aggravate rosacea and cause interdependence.
Systemic treatments
Here, it is possible to distinguish the antibiotics of the tetracycline family. There are several molecules: lymecycline (300 mg/d) and doxycycline (100 mg/d).
In some parts of the world, only doxycycline has received marketing authorization. These medications will reduce the papules, pustules and also the ocular symptoms of rosacea. So these are not treatments intended to cure the disease, but rather to suspend it.
In the event that antibiotics prove to be poorly tolerated or ineffective, isotretinoin can be used. This is a vitamin A derivative that has an anti-inflammatory action.
In France, it can be had in four generics: Isotretinoin TEVA, Procuta® Gé, Curacné® Gé and Contracné® Gé.
For women of childbearing age, isotretinoin must be combined with an oral contraceptive to avoid pregnancy. It is formally contraindicated for pregnant women, as it increases the risk of birth defects.
In view of all these indications, the prescription of isotretinoin should be made under close medical supervision, by a dermatologist only.
The pharmacist cannot dispense this medication if the prescription is from a physician other than a dermatologist. In addition, medical monitoring involves regular – monthly – pregnancy tests to ensure that the patient has not become pregnant in the interim.
Redness and vascular spot treatments
To effectively eliminate vascular spots and telangiectasias (there are other transient rednesses that do not require laser treatment to disappear), it is possible to opt for IPL treatment (intense, pulsed lamps) or laser.
A distinction is made between pulsed dye lasers and KTP lasers.
The duration of treatment varies depending on the device used and the setting chosen by the practitioner.
It typically takes 2-6 laser sessions to eliminate 60-80% of redness.
Laser treatment can be a bit painful, but the pain is usually bearable. Also, for results to be visible, it is usually necessary to wait two months after the series of treatment sessions.
CO2 laser surgery is the most appropriate treatment for rhinophyma.
Treatment of ocular rosacea
First and foremost, obtain an ophthalmologic consultation to determine the presence of keratitis. The antibiotics listed above may then be recommended.
As noted in the paragraph on ocular rosacea, there may be conjunctivitis or blepharitis.
In these cases, eye care is necessary. Ophthalmic baths and eye humectants such as Celluvisc® are most helpful.
Treatment is then symptomatic and includes the application of artificial tears to combat xerophthalmia (dry eye).
Complementary cosmetic care
Here, it is possible to distinguish, among others, the anti-redness creams Eucerin, Créaline AR or even Rosaliac.
These cosmetics can be used to moisturize the skin, increase comfort and follow-up treatments. Their tolerance on the body helps to improve burning sensations.
They are usually composed of a sunscreen and are used to mask distressing lesions and redness.
It is also possible to use foundation to mask redness.
Note, however, that scented creams should be avoided: for daily facial cleansing, it is better to prefer unscented cleansers such as an Avene micellar solution or physiological Crealine TS from Bioderma.
It is essential to use a high protection SPF 50 sunscreen to prevent redness from worsening due to the sun or to avoid aggravating situations related to taking photosensitizing antibiotics.